

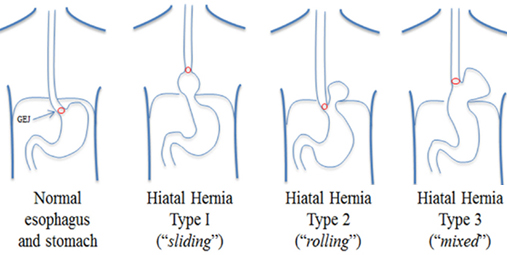
The gorge passes through a gap within the diaphragm (i.e. esophageal hiatus) because it courses through the chest to the abdomen eventually ending at the abdomen. This gap is sometimes adequate for passage of the gorge and zilch else. However, patients that have a hernia have AN enlarged gap. Their square measure four different types of hiatal hernias delineate. The slippery herniation is that the most typical of the four representing quite eighty-percent of all hiatal hernias. The lower muscle system sphincter- the air mass zone close to the junction of the abdomen and gorge- fails and permits abdomen contents to reflux into the esophagus. Dr. PS Lubana cures as Laparoscopic Hernia Surgeon in Indore at apple hospital.
Several studies are helpful to your doctor in making the diagnosis of hiatal hernia including:
Laparoscopic Cruroplasty and Nissen fundoplication is that the procedure of selection for repair of a hernia. Patients that have para-esophageal herniation that permits the structure to be displaced into the chest on top of the GE junction or patients with alternative abdominal organs (e.g. spleen, colon, liver) displaced into the chest ought to be repaired desperately. Repair can facilitate forestall complications like hurt, enteric disruption, strangulation and therefore the like. Elective repair is suggested just for patients that square measure well and have a slippery herniation. This cluster of good patients may additionally be followed clinically seeking surgery only symptoms arise.
In the past, open surgery was the sole choice for repair. This approach is related to prolonged recovery time and an oversized painful incision. With the new minimally invasive approach, surgery is currently a viable initial medical aid even for patients .
The laparoscopic cruroplasty and Nissen fundoplication are performed through 5 quarter-inch incisions through that, a camera and instruments square measure placed. The herniation is reduced from the chest into the abdomen. This may need separation of abdominal organs from the respiratory organ and middle chest structures. The hiatus is then re-approximated to the acceptable size. Some hernias square measure therefore massive and tissues square measure therefore poor that prosthetic material should be accustomed forestall repetition. After adequate repair of the hiatus, a brand new lower muscle system valve is made by wrapping a two-centimeter portion of the abdomen around the lowermost portion of the gorge. This collar is then anchored to the tough fibers of the diaphragm. The procedure generally lasts for 2 to four hours betting on the scale and contents of the herniation. Patients square measure started on clear liquids future morning and square measure discharged within the afternoon. The open surgical technique involves AN 8-10 in. higher abdominal incision with a hospital keep of 5-7 days. Dr. Frantzides initiated and completed a ten-year prospective irregular study within which he enclosed patients United Nations agency underwent laparoscopic hernia repair with and while not mesh. He found that rather than a 20-35% repetition rate the employment of mesh would cut back or eliminate recurrences. This study was revealed in 2002 within the Archives of Surgery.
Patients recover sooner once laparoscopic cruroplasty and Nissen fundoplication. Return to activities will occur inside 2-7 days compared to 4-6 weeks with AN open approach. Wound infections occur less oft with the laparoscopic technique. Also, less pain has been reported with laparoscopy. Most significantly, larger than ninety-percent of patients square measure symptom-free 10 years once the procedure.



© Dr. Parvinder S. Lubana. All rights reserved. | Developed & Design by ipromptsolution.com